62 Watts Street:
Modeling the Backdraft
Thursday, March 26th, 2009
On March 24, 1994 Captain Drennan and Firefighters Young and Seidenburg of the FDNY were trapped in the stairwell of a three-story apartment building �by rapid fire progression that occurred as other companies forced entry into the fire apartment on the floor below. The FDNY requested assistance from National Institute for Standards and Technology (NIST) in modeling this incident to develop an understanding of the extreme fire behavior phenomena that occurred in this incident.
Brief Review
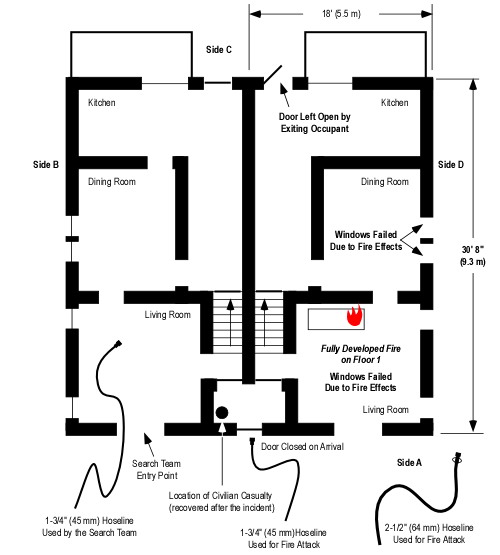
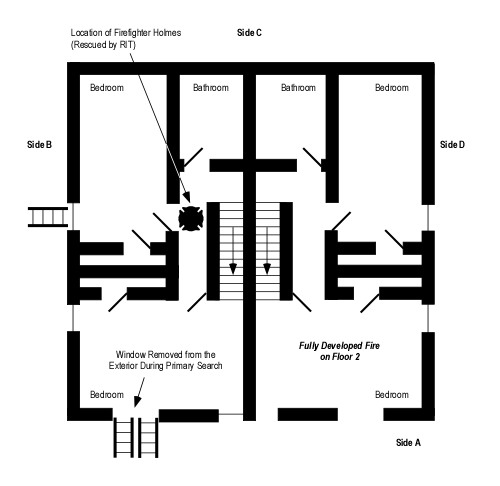
A short case study of the 62 Watts Street incident was presented in my last post. As a brief review, FDNY companies responded to 62 Watts Street for a report of smoke and sparks coming from the chimney (see Figure 1). On arrival, there was no indication of a serious fire in the building. Companies opened the scuttle over the stairwell and stretched a line to the first floor apartment while Captain Drennan and the other members of the Ladder 5’s inside team proceeded to the second floor to search for occupants. When the door to the first floor apartment was opened, air rushed in and then warm smoke pushed out. This pulsation in the air track at the door was followed by a flaming combustion filling the upper portion of the door and almost immediately filling the stairwell. Firefighters on the first floor were able to escape, while Captain Drennan and Firefighters Young and Seidenburg were trapped on floor 2.
Figure 1. 3D Cutaway View of 62 Watts Street

Analysis and Computer Modeling
FDNY asked NIST to assist in developing a computerized model to aid developing an understanding of the fire behavior phenomena that occurred during this incident.
Hypothesis: The fire burned for over an hour under severely ventilation controlled conditions resulting in production of a large quantity of unburned pyrolyzate and products of incomplete combustion. Opening the apartment door allowed exhaust of warm fire gases and inflow of cooler ambient air, resulting in a combustible fuel/air mixture. Bukowski (1995) does not identify a source of ignition. However, it is likely that the combustible fuel/air mixture underwent piloted ignition as flaming combustion resumed in the apartment. Once the gas phase fuel was ignited, flaming combustion extended from the door through the stairwell to the ventilation opening at the roof.
Richard Bukowski of the NIST Building and Fire Research Laboratory modeled the fire using CFAST to determine if a sufficient mass of gas phase fuel could have accumulated in the apartment to account for the severity and duration of flaming combustion that occurred. CFAST is a two-zone fire model used to predict the distribution of smoke and fire gases and temperature over time in a multi-compartment structure subjected to a fire. A two-zone model is based on calculations that describe conditions in the upper and lower layers (see Figure 2). While there are obvious differences in conditions within each of these zones, these differences are relatively small in comparison to the differences between the two zones (Jones, Peacock, Forney, & Reneke, 2005).
Figure 2. Upper and Lower Layers in Two Zone Models

Bukowski’s (1995) model of the Watts Street fire divided the involved area of the structure into three compartments. The apartment was defined as a single 6.1 m (20′) x 14 m (46′) x 2.5 m (8’3″) compartment. The stairwell was defined as a second 1.2 m (4′) x 3 m (10′) x 9.1 m (30′) compartment connected to the apartment by a closed door and having a roof vent with a cross sectional area of 0.84 m2 (9 ft2). The fireplace flue was defined as a vertical duct with a cross section of 0.14 m (1.5 ft2) x 10 m (33′).
The heat release rate in the initial growth phase of a compartment fire is nearly always accelerating with energy release as the square of time (t2). Multiplying t2 by a factor ?, various growth rates (e.g., ultra-fast, fast, medium, slow) can be simulated (Karlsson & Quintiere, 2000).
Based on experimental data from burning trash bags, Bukowski (1995) estimated the initial heat release rate at 25 kW with the fire transitioning to a medium t2 fire (typical of residential structure contents) which would have had a peak HRR of 1 MW, but did not reach this HRR due to limited ventilation.
Figure 3. Heat Release Rate of Growth Phase t2 Fires.

Note: Adapted from CFAST – Consolidated model of fire growth and smoke transport (Version 6).
Results of the computer model indicated that the HRR of the fire in the apartment grew to a heat release rate of 0.5 MW (see Figure 4) and then HRR decreased rapidly as oxygen concentration dropped below 10% (see Figure 5).
As the fire continued to burn under extremely ventilation controlled conditions, the concentration of unburned pyrolizate and flammable products of incomplete combustion in the apartment continued to increase.
Figure 4. Heat Release Rate

Note: Adapted from Modeling a Backdraft: The 62 Watts Street Incident.
Research indicates that the concentration of gas phase fuel (e.g., total hydrocarbons, carbon monoxide) is a critical determinant in the likelihood of backdraft occurrence. In small scale, methane fueled compartment fire experiments, Fleischmann, Pagni, & Williamson (1994) found that a total hydrocarbon concentration >10% was necessary for occurrence of a backdraft.� At lower concentrations, flame travel is slow and compartment overpressure is lower. As total hydrocarbon concentration increased, the overpressure resulting from backdraft increased. Similarly, Weng & Fan (2003) found mass fraction (concentration by mass) of unburned fuel to be the critical determinant in the occurrence and severity of backdraft. In their small scale, methane fueled experiments, increases in mass fraction of unburned fuel resulted in increased overpressure and more severe backdraft explosions.
Both of these research projects involved use of a methane burner in a compartment and the researchers identified the need for ongoing research using realistic, full scale compartment configurations and fuel loads.
Figure 5. Oxygen Concentration

Note: Adapted from Modeling a Backdraft: The 62 Watts Street Incident.
Figure 6. Temperature

Note: Adapted from Modeling a Backdraft: The 62 Watts Street Incident.
Estimating the time that fire companies forced the door to the apartment, the front door in the simulation was opened at 2250 seconds. As in the actual incident, there was an outflow of warm air from the upper part of the doorway, followed by inward movement of ambient air in the lower part of the doorway. Almost immediately after this air track pulsation, the heat release rate in the stairwell increased to nearly 5.0 MW (see Figure 5), and raising temperature in the stairwell to in excess of 1200o C (2200o F).
Theory and Practice
Output from the CFAST model was consistent with the observation and conditions encountered by the companies operating at 62 Watts Street on March 28, 1994.� The model showed that sufficient fuel could have accumulated under the ventilation controlled conditions that existed in the tightly sealed apartment to result in the extended duration and severity of flaming combustion that occurred in the stairwell.
Following this investigation, FDNY identified a number of similar incidents that had occurred previously, but which had gone unreported because no one had been injured. Remember that it is important to examine near miss incidents as well as those which result in injuries and fatalities.
Questions
The following questions focus on fire behavior, influence of tactical operations, and related factors involved in this incident.
- Examine the oxygen concentration and temperature curves (Figures 5 & 6) up to the time that the door of the apartment was opened (2250 seconds). How does this data fit with the observations of the company making entry into the first floor apartment and your conception of conditions required for a backdraft?
- How might the temperature in the apartment have influence B-SAHF indicators visible from the exterior an when performing door entry during this incident?
- In Modeling a Backdraft Incident: The 62 Watts St (NY) Fire, Bukowski (1995) states “as buildings become better insulated and sealed for energy efficiency such hazards [e.g., ventilation controlled fires, increased concentration of gas phase fuel, backdraft] may become increasingly common. Thus, new operational procedures need to be developed to reduce the likelihood of exposure to flames of this duration” (p. 5) What operational procedures and practices would be effective in reducing risk and mitigating the hazards presented by ventilation controlled fires in energy efficient buildings? Consider size-up and dynamic risk assessment as well as strategies and tactics.
- The often oversimplified tactical approach to dealing with potential backdraft conditions is to ventilate vertically. In this case, existing roof openings were used to ventilate the stairwell, but this had no impact on conditions in the apartment. How can tactical ventilation be used effectively (or can it) when faced with potential backdraft conditions on a lower floor or in a basement?
- Another, less common approach to dealing with potential backdraft conditions is to cool the atmosphere and� inert the space with steam to reduce the potential for ignition. Examine the temperature curve prior to opening of the door (2250 seconds) and determine if this was a viable option?
- Bukowski’s (1995) paper did not speak to the door entry procedures used by the companies at the apartment door. How might good door entry procedures have reduced risk in this incident?
Ed Hartin, MS, EFO, MIFIreE, CFO
References
Bukowski, R. (1996). Modeling a backdraft: The 62 Watts Street incident. Retrieved March 14, 2009 from http://fire.nist.gov/bfrlpubs/fire96/PDF/f96024.pdf
Fleischmann, C., Pagni, P., & Williamson, R. (1994) Quantitative backdraft experiments. Retrieved March 15, 2009 from http://www.fire.nist.gov/bfrlpubs/fire94/art135.html
Jones, W., Peacock, R., Forney, G., & Reneke, P. (2005). CFAST – Consolidated model of fire growth and smoke transport (Version 6) Retrieved March 15, 2009 from http://cfast.nist.gov/Documents/SP1026.pdf.
Karlsson, B. & Quintiere, J. (2000). Enclosure fire dynamics. New York: CRC Press.
Weng, W. & Fan, W. (2003). Critical condition of backdraft in compartment fires: A reduced scale experimental study. Journal of Loss Prevention in the Process Industries, 16, 19-26.