Reading the Fire: B-SAHF
November 24th, 2008Surprises are Bad!
I frequently observe that surprises on the fireground are bad. Unexpectedly worsening conditions can place firefighters at risk and often result in injuries and fatalities. However, event unexpected success can be problematic, as we don’t know why we were successful (and will likely attribute it to our mastery of the firefighting craft). When we are surprised by fire development or the effectiveness or ineffectiveness of our tactical operations, we really don’t know what is going on! Recognizing critical fire behavior indicators and being able to predict likely fire behavior is a critical skill for firefighters and fire officers at all levels.
B-SAHF: A Systematic Approach
In his paper Reading the Fire Station Officer Shan Raffel of Queensland Fire Rescue observed:
Every fire sends out signals that can assist the firefighter in determining the stage of fire development, and most importantly the changes that are likely to occur. This skill is essential to ensure the correct firefighting strategy and tactics are employed. Being able to “read a fire” is the mark of a firefighter who is able to make decisions based on knowledge and skill, not guess work or luck.
Shan developed a scheme for organizing critical fire behavior indicators that focused on Smoke, Air Track, Heat, and Flame (SAHF). As we worked together in refining this system, I found that one element was missing, the building. Adding building factors that influence fire behavior provides a reasonably comprehensive approach to reading the fire to identify the stage of fire development, burning regime, and likely fire behavior. The simple mnemonic B-SAHF (Building-Smoke, Air Track, Heat, & Flame) can be used to remember this simple approach to reading the fire.
B-SAHF Indicators
The fire behavior indicators should not be considered as a checklist as key indicators will vary with incident conditions. Look at fire behavior indicators from a holistic perspective as illustrated by the following concept map:
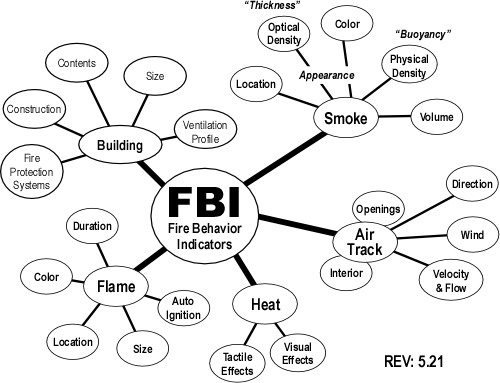
Note: This concept map only illustrates the second level of detail in examining the B-SAHF indicators. It is important to extend this map by adding additional detail in each of the categories. For example, in building factors, size may be expanded to include building area and height, number of stories, internal compartmentalization, etc. For a more detailed look at B-SAHF, down load a copy of the full version of B-SAHF Version 5.2.1 in PDF format.
Building: Many aspects of the building (and its contents) are of interest to firefighters. Building construction influences both fire development and potential for collapse. The occupancy and related contents are likely to have a major impact fire dynamics as well.
One of the key factors related to building factors is that they are present before the fire starts. Fire behavior prediction (at least in general terms) should be a key element in pre-incident planning. Look at the building and visualize how a fire would develop and spread based on key building factors.
Smoke: What does the smoke look like and where is it coming from? This indicator can be extremely useful in determining the location and extent of the fire. Smoke indicators may be visible on the exterior as well as inside the building. Don’t forget that size-up and dynamic risk assessment continue after you have made entry!
Air Track: Related to smoke, air track is the movement of both smoke (generally out from the fire area) and air (generally in towards the fire area). Observation of air track starts from the exterior but becomes more critical when making entry. What does the air track look like at the door? Air track continues to be significant when you are working on the interior.
Heat: This includes a number of indirect indicators. Heat cannot be observed directly, but you can feel changes in temperature and may observe the effects of heat on the building and its contents. Remember that you are insulated from the fire environment, pay attention to temperature changes, but recognize the time lag between increased temperature and when you notice the difference. Visual clues such as crazing of glass and visible pyrolysis from fuel that has not yet ignited are also useful heat related indicators.
Flame: While one of the most obvious indicators, flame is listed last to reinforce that the other fire behavior indicators can often tell you more about conditions than being drawn to the flames like a moth. However, that said, location and appearance of visible flames can provide useful information which needs to be integrated with the other fire behavior indicators to get a good picture of conditions.
It is important not to focus in on a single indicator, but to look at all of the indicators together. Some will be more important than others under given circumstances.
Exercising Your Skills
Learning to read the fire takes practice and a solid understanding of practical fire dynamics. This post introduces the concept of B-SAHF and the B-SAHF exercise as a method for improving your skill in reading the fire.
Download and print the B-SAHF Worksheet and then view the first 45 seconds of the following video of an apartment fire in New York City. First, describe what you observe in terms of the Building, Smoke, Air Track, Heat, and Flame Indicators. Second, answer the following five questions:
- What additional information would you like to have> How could you obtain it?
- What state(s) of fire development is the fire likely to be in (incipient, growth, fully developed, or decay)? Remember that fire in adjacent compartments can be in a different stage of development?
- What burning regime is the fire in (fuel or ventilation controlled)?
- What conditions would you expect to find inside this building?
- How would you expect the fire to develop over the next two to three minutes
Find more videos like this on firevideo.net
After completing the B-SAHF exercise, view the remainder of the video. Did you successfully predict the fire behavior that occurred? What conditions do you think the firefighters encountered on the interior of the structure?
Now What?
Developing skill in reading the fire requires practice. Additional B-SAHF exercises will be posted on a regular basis at cfbt-us.com. If you have a video clip or photo that you would be willing to share for a B-SAHF exercise, please visit the Contact Us page and send me an e-mail. Also check the CFBT-US Resources page for additional information on Reading the Fire!
Additional Information on Loudoun County Flashover
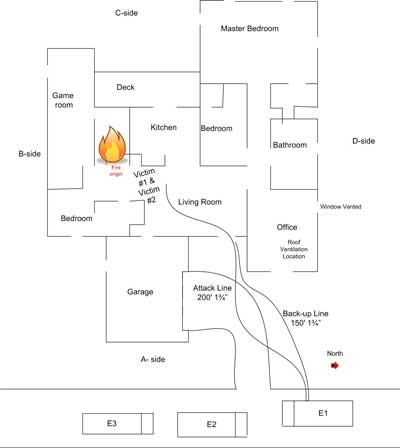
Previous posts examined an incident in which a number of Loudoun firefighters were injured in a flashover. See Loudoun County Virginia Flashover, Loudoun County Flashover: What Happened, and Loudoun County Flashover: Escape from Floor 2. Several weeks ago Loudoun County Fire, Rescue, & Emergency Management released a presentation including video shot by a civilian bystander during the incident. Print a second copy of the B-SAHF Worksheet and view the Meadowood Court Video, using the worksheet to examine the fire behavior indicators visible from the exterior.
Loudoun County Fire, Rescue, & Emergency Management has also made this video available for download: Meadowood Courth Video Download.
Ed Hartin, MS, EFO, MIFireE, CFO